What is Fundoplication?
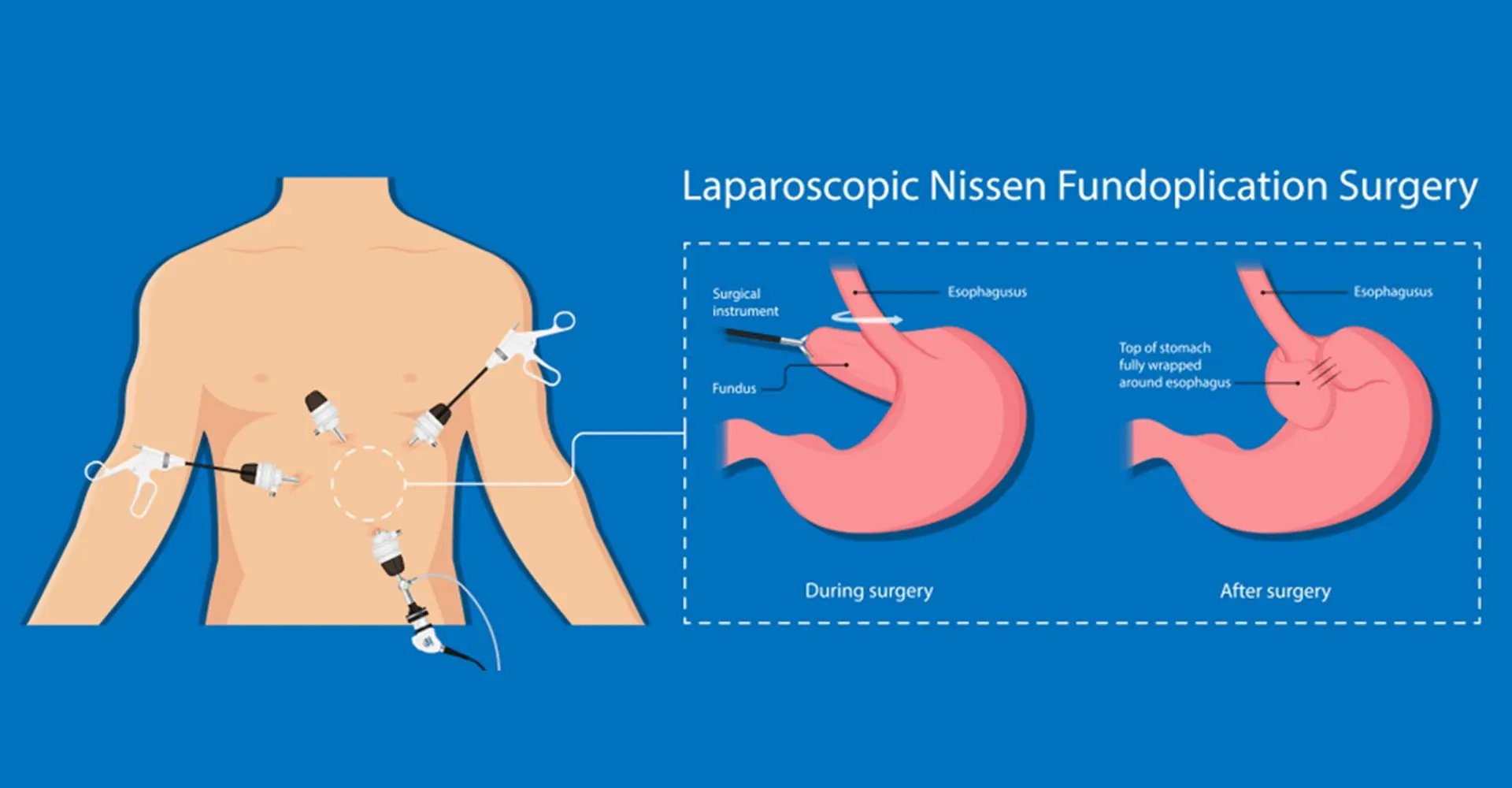
Laparoscopic anti-reflux fundoplication in Merida is the definitive surgical solution for severe gastroesophageal reflux disease (GERD) that does not respond to medications. GERD affects 10-20% of the adult population, and in severe cases can progress to erosive esophagitis, Barrett's esophagus, and ultimately esophageal cancer. The procedure wraps the gastric fundus around the lower esophagus to reconstruct the lower esophageal sphincter, the natural barrier that prevents reflux. The most common technique is Nissen fundoplication (360° wrap); in selected cases, Toupet fundoplication (270°) is used to reduce the risk of postoperative dysphagia. The surgery also corrects the hiatal hernia when present, resolving the underlying anatomical defect. Anti-reflux surgery specialist in Merida offers this proven laparoscopic treatment for patients throughout Yucatan.
Dr. Mario Ruvalcaba performs laparoscopic fundoplication in Merida through 4 to 5 small incisions under general anesthesia. Surgery lasts 1.5 to 2.5 hours. The indication requires objective confirmation of GERD through 24-hour pH-metry and/or esophageal manometry, upper digestive endoscopy, and in some cases upper GI series. Hospital discharge is given the following day or within 48 hours with an initial liquid diet.
Certified by the Mexican Council of General Surgery with more than 5 years of experience in laparoscopic esophagogastric surgery in Merida, Dr. Ruvalcaba performs complete functional esophageal evaluation before surgery to correctly classify GERD and select the most appropriate technique. He operates at the leading hospitals in Merida, Yucatan, with the diagnostic and therapeutic resources needed for complex esophageal pathology management.
More than 90% of patients achieve complete reflux elimination after fundoplication, with symptom resolution, esophagitis improvement, and the possibility of discontinuing proton pump inhibitors. Full functional recovery is achieved within 4 to 8 weeks. If you have severe reflux that medications cannot control, a permanent solution exists. Schedule your consultation today.
Benefits
Definitive Solution
Permanently eliminates gastroesophageal reflux in more than 90% of patients, avoiding lifelong medication dependence.
Prevention of Complications
Stops the progression of esophagitis, reduces the risk of Barrett's esophagus and its complications, and improves quality of life comprehensively.
Medication Independence
The vast majority of patients can discontinue proton pump inhibitors after surgery.
Minimally Invasive
Laparoscopic approach with 1 to 2 week recovery, without the morbidity of conventional open surgery.
Who Is a Candidate?
- ✓Patients with severe GERD confirmed by 24-hour pH-metry and/or esophageal manometry, with symptoms not adequately controlled with proton pump inhibitors.
- ✓Individuals with grade C or D esophagitis (Los Angeles), Barrett's esophagus, or peptic stricture requiring definitive reflux correction.
- ✓Patients with sliding or paraesophageal hiatal hernia contributing to reflux and causing symptoms such as heartburn, regurgitation, dysphagia, or respiratory symptoms.
- ✓Individuals who prefer a definitive surgical solution over long-term medication dependence, after appropriate evaluation confirming they are suitable candidates.
- ✓Patients with laryngopharyngeal reflux or extraesophageal reflux manifestations (chronic cough, hoarseness, asthma, dental erosion) refractory to medical treatment.
Recovery Process
First week
Strict liquid diet for the first 7 days to allow healing of the repair and adaptation to the new anatomy. There may be temporary dysphagia (difficulty swallowing), especially for solids. The patient returns home the following day or within 48 hours.
2–4 weeks
Gradual progression to soft diet and then solid foods. Dysphagia gradually resolves. It is recommended to eat slowly, chew well, and avoid large bites. Return to sedentary activities around day 10.
1–3 months
Complete adaptation to the new anatomy. Most patients can eat all foods normally. Reflux symptoms should be completely resolved. During this period, a control endoscopy is performed to verify esophageal healing.
6–12 months
Full recovery. Follow-up to confirm absence of reflux recurrence and resolution of esophagitis or Barrett's when present. Patients with Barrett's require subsequent periodic endoscopic surveillance.
Frequently Asked Questions about Fundoplication
When is anti-reflux surgery indicated instead of medications?
Surgery is indicated when reflux is severe and not adequately controlled with optimal doses of proton pump inhibitors, when the patient does not wish to take lifelong medication, when reflux complications are present (severe esophagitis, Barrett's, stricture), when there is a large hiatal hernia, or when reflux generates extraesophageal manifestations (cough, hoarseness, asthma).
What is postoperative dysphagia and how long does it last?
Dysphagia (difficulty swallowing) is the most common side effect after fundoplication and occurs to varying degrees in most patients during the first 4 to 8 weeks. It is caused by postoperative edema and inflammation and by adaptation to the new anatomy. In the vast majority of cases it resolves spontaneously between weeks 4 and 8 with an appropriate diet.
Can fundoplication be performed if I have a large hiatal hernia?
Yes, in fact hiatal hernia repair is an integral part of the anti-reflux procedure. In large paraesophageal hernias (type III and IV), surgery is scheduled electively to repair the defect and reposition the stomach in the abdomen, combining crural repair with fundoplication.
Can reflux return after surgery?
The reflux recurrence rate at 10 years is 10 to 15%, generally due to progressive relaxation of the fundoplication or recurrent herniation. However, the vast majority of patients maintain excellent long-term results, with more than 85% reporting complete satisfaction at 10 years after surgery.
How much does laparoscopic fundoplication cost in Merida?
The cost varies based on the hospital and required preoperative studies (pH-metry, manometry, endoscopy). Dr. Ruvalcaba provides a detailed quote during the initial consultation. Many medical insurance plans cover fundoplication when there is documented medical indication with esophageal functional studies. Consult with your insurer and the office for more information.
How long does laparoscopic fundoplication take?
Laparoscopic fundoplication takes 1.5 to 2.5 hours under general anesthesia. In cases that include large hiatal hernia repair, additional time may be required. Hospital discharge is given the following day or within 48 hours, with strict liquid diet for the first 7 days.
When can I return to work after fundoplication?
Patients with sedentary or office work typically return around day 10 postoperatively. The most important restriction during the first 2 weeks is dietary: liquid then soft diet to allow healing. For physical work, 3 to 4 weeks of rest is recommended. Temporary dysphagia gradually resolves between weeks 4 and 8.
This content is for informational purposes only and does not replace a medical consultation.